Oh The Damage Done
“I hit the city and
I lost my band
I watched the needle
Take another man
Gone, gone, the damage done.” Neil Young, “The Needle and the Damage Done.”
Two years ago I wrote a report on the annual economic impacts of drug and alcohol abuse in New Hampshire. It surprised many (and probably created much skepticism) with its findings of $1.84 billion in costs in 2012. Since my analysis of 2012 data the number of drug induced deaths in New Hampshire has almost doubled, from just over 200 to 400 and there is a greater awareness of the damage done in the state by drug abuse.

What surprised me in 2014 was how much more advanced the data on the incidence of alcohol abuse and its negative impacts was than was the data on the incidence and negative impacts associated with drug abuse. I felt strongly then that my estimates of the costs of drug abuse were understating its true costs and I feel even more strongly about that today. Research on the negative impacts of alcohol use is more extensive, in part, because alcohol abuse affects more individuals and more individuals across a broader spectrum of the population. In addition, alcohol abuse has been identified as a major economic and societal issue for a much longer period of time. But I also think the relative lack of data and research on the societal and economic costs of drug abuse is, in part, a function of a tacit belief that drug abuse was largely a problem confined to individuals on the margin of society as well as some celebrities. In contrast, alcohol abuse has long been recognized as an affliction that does not discriminate along social, economic, or demographic lines. When the effects of drug abuse (or domestic abuse, human trafficking etc.) are seen to be confined to more marginal members of society it is easier to assign it a lower priority in the long list of public issues that should to be addressed. Increasingly common media reports about the dramatic rise in drug induced deaths, and drug use among a broader segment of society in New Hampshire and nationally, have raised the public’s (and policymakers’s) awareness of the socioeconomic breadth of the issue that long preceded the media’s attention. I couldn’t do my job well if I didn’t approach every analysis and every research project dispassionately but it is more than a little discomforting to me that our hearts today seem to be running around inside of reporters and journalists.
Me and my friends and colleagues in the business community frequently lament the fact that New Hampshire has among the highest electricity costs and highest business tax rates of any state in the nation, as well as the impacts that each has on NH’s economy. We should also be outraged by the fact that NH has the third highest rate of drug induced deaths per 100,000 residents among the 50 states, the tremendous costs that are associated with those deaths, as well as the costs associated with thousands of other users in the state who have not yet died from abusing drugs.
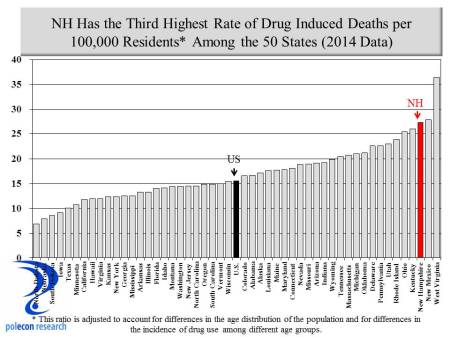
The rates in the chart are age adjusted, meaning they are adjusted to reflect difference in the age composition of each state’s population. In the same way the rate of heart attack deaths per 100,000 in a state like Florida (a state with more older residents) would be expected to be higher than in a state like Utah (the youngest state by median age), a younger state would be expected to have higher rates of drug induced deaths. New Hampshire is not a young state so our 400 drug induced deaths among our population creates a staggeringly high ratio given the composition of our population.
Maybe the hearts of most of the members of the business community are inside of accountants (as if they have hearts) rather than journalists: we should find out as the economic costs of drug abuse continue to rise.
Explore posts in the same categories: Drug Abuse, DrugsTags: Cost of Drug Abuse, Drug Abuse, Drugs, NH
You can comment below, or link to this permanent URL from your own site.
February 1, 2016 at 1:55 pm
More good work! But, until the state invests some money in treatment capacity, the numbers will continue to rise. By the way, have you ever asked yourself why doctors, who presumably have known for more than a century that opiates (1) ease pain and (2) are addictive, began prescribing them like candy?
February 1, 2016 at 3:00 pm
Thanks for the kind words about the post Mike. My report noted the low level of treatment expenditures in NH. Over one-half of treatments in NH are paid for “out-of-pocket”, no doubt lowering the number in treatment and the number of treatment facilities. And yes the physician issue is one that is drawing more and more attention as a contributing factor to the problem.
February 1, 2016 at 2:40 pm
Our quest for happiness and pain averse culture, where a pill is often the first choice to address mental or physical pain, has created this demand for opiates. Education needs to begin before a person goes into a Dr’s office, so that our path of dependency might not even have to begin.
February 1, 2016 at 3:09 pm
I agree Muriel. Sad there seems to be so little joy in world or so many people can’t find it that they turn to psychoactive substances. I never really understood the desire or need for such substances and I came of age during a time when it was increasingly rampant. Time with my kids, hiking with my dog, building or repairing anything, and perhaps too often a well-oaked chardonnay (yes I know that can include me in “the problem”) make my quest for happiness a relatively easy task.
February 1, 2016 at 7:21 pm
Michael Kitch – does treatment work? I have been a psychiatric social worker for almost four decades and don’t see evidence that most substance abuse treatments have any effect. They make providers feel better.
Similarly, Muriel – what education are you thinking of that does not already exist? Schools have been chockablock full of antidrug education for decades.
I wish I had answers. I am not just trying to share my discouragement. But assuming we know what will work is what drives expensive useless solutions.
February 1, 2016 at 7:54 pm
Thanks for taking the time to read this post and especially to provide a thoughtful comment. I don’t want to answer for Micheal (but I don’t think he can respond) and I am no expert on treatment but I did see see studies citing some pretty high effectiveness rates for some treatments. Regardless, we didn’t stop trying when cancer treatment and survival rates were abysmal decades ago – at the time you could have argued that treatments back then, with their low success rate, were “expensive useless solutions”.
February 1, 2016 at 8:09 pm
Dennis Sasseville sent me the post and assures me you like data (and I forwarded this to a data driven friend who is a researcher at Dana Farber now.). I don’t want to send you scurrying, but if you run across encouraging treatment data again, post it, as I have checked to follow the thread. But frankly, I’m betting not. It has been my daily bread for years. Disease solutions have to involve admitting things don’t work and going on to something else. There isn’t much of trying anything new, just lobbying for more of the same. Genetically identifying probably addicts is about the best we’ve got – and that has some frightening possibilities. (And some good ones, maybe.)
There is confirmation bias all over the research in substance abuse treatment. Alan Green up at Dartmouth is one of the few I trust, and he is not cheery.
February 1, 2016 at 8:42 pm
Thanks for the stats lesson as well as your anecdotal insights.
February 1, 2016 at 8:57 pm
Sorry if I sounded snippy.
February 1, 2016 at 9:16 pm
No problem but you shouldn’t dismiss Dennis’ assessment of my skill set. He is a wise and good man and clearly a keen judge of ability.
February 1, 2016 at 9:24 pm
I think that the public education is focused on the illegal, scary drugs and that no one has taken on education about the over dependency on prescriptions…that of course would go against drug companies’ advertisements and the “Dr. knows best” culture. Personal responsibility (first) in healing oneself is not the easy way out, in our easy way out culture…..
February 1, 2016 at 7:22 pm
BTW – I used to do backup vocals in a band that did that Neil Young song. Thanks.
February 1, 2016 at 7:58 pm
A great song, a bit before my time (I vaguely remember it from my youth but really had no idea what it was referencing). I appreciated it later in life. Now if you ever sang any Levon Helm song then you have the right to post anything you want on my blog.
February 1, 2016 at 7:56 pm
Does NH track these deaths by town or region? I know MA does, and there’s some pockets that are much worse than others. I think this is important data, and it is sometimes more easily grasped if you can see how it’s effecting your town or the town next to you.
Example here for opioid death rates (not age adjusted):
https://www.bostonglobe.com/metro/2015/10/22/town-town-look-opioid-epidemic-deadly-toll-massachusetts/FJksUU8hlYJN4Yl4mCKwkI/story.html
February 1, 2016 at 8:05 pm
Hi,
Thanks for the link. I am sure NH does track by town and region, they produce mortality and birth data by town. NH isn’t very good at making state available in a timely and easily accessible form however (I say this as someone who has done projects in dozens of states). The data in this post is from the CDC (as reported to them by NH officials) which is more limited in geographic breakdown but does allow for age and othjer demographic breakdowns.
February 1, 2016 at 9:05 pm
Thanks! I’m glad I’m not missing something with NH data. The few times I’ve tried to find anything I’ve come up short. The closest I could find here was that about 75 deaths were in Manchester alone. Curious if the major driver is the Manchester/Nashua rates or if the spike represents a move in to the smaller towns.
Anyway, thanks for the post and reply!